Glaucoma a public health problem of growing importance.
As more and more people live longer as medical facilities improve so does glaucoma become more of a public health problem?
Consider this- In the USA alone, more than 25 million people have a significant visual loss, and over 150,000 people are blind in both eyes due to it. Worldwide, studies found that More than 5 million people are blind in both eyes from glaucoma. Considering that our population is so large we can safely estimate that more than 3 crore people in the country have the disease!
Glaucoma is not a new ailment The word glaucoma came from ancient Greek,(Hippocrates 400BC) meaning a cloudy blue-green hue, most likely describing a person with a swollen cornea or who was rapidly developing a cataract, both of which may be caused by long-standing high pressure inside the eye.
These ancient surgeons told of a “tightness” and “whitening” of the eye, of “black water”, that filled inside the eye robbing the patient of sight. To this day across India, people refer colloquially to this as “ Kala Motia” or in Gujarati as “Jhamar.”
Glaucoma is a public health problem in India today.
.

The most common symptoms are,
- Frequent change of glasses (none of which is satisfactory)
- Difficulty in dark adaptation
- Bumping into things at unfamiliar places.
- Blurred or foggy vision.
- Colored halos (rainbow-colored rings) around lights.
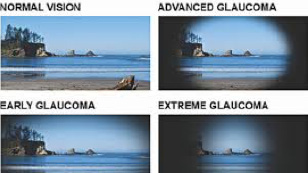
This is an example of a normal vision.
This is also an example of how someone sees during the beginning stages of open-angle glaucoma. Because there are no symptoms initially, regular eye examinations are very important.
Early symptoms may include a gradual and often imperceptible failing of peripheral (side) vision.
As the disease progresses, the center of vision may still be clear, however, peripheral vision begins to fail.
During the advanced stages of glaucoma, only a small central area of vision remains. If the entire optic nerve is destroyed, then total blindness will result.
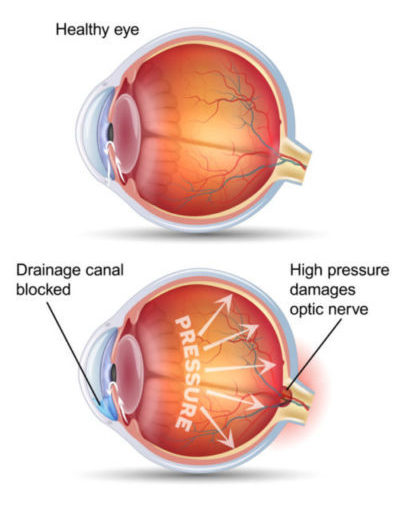
The human eye has a part called the ciliary body that produces a fluid called “Aqueous”. This aqueous has to flow out of the eye through a mesh similar to a tea strainer.
This mesh is called the trabecular meshwork. With age, injury, diabetes, swelling, cataract, bleeding in the eye, etc the mesh gets blocked leading to a rise in pressure in the eye. This rise in pressure presses on the optic nerve inside the eye. The peripheral vision (side vision)decreases. However, there is usually no pain and central vision is preserved to the end. Since central vision and reading vision is preserved until the disease is very severe, it usually slips the patients attention and is detected accidentally by the ophthalmologist when the person visits them for some other eye complaint.
Glaucoma there must consist of 3 basic documented findings
- Increased pressure in the eye (normal is usually taken as less than 21 millimeters of mercury)-sometimes pressure may be normal which does not preclude the diagnosis!
- Optic nerve changes which are seen by your eye doctor by looking inside the eye and documenting it with a picture. Nowadays an AngioOCT device has supplanted the taking of pictures.
- Loss of “field” or side vision. -Important.
Remember, Open-Angle Glaucoma is a Painless disease and the only clue the patient has is sometimes a dull headache or sudden increase in reading number.
Stents:
The pressure can be checked by a machine called a “tonometer” Modern set-ups must have a computerized device that blows a puff of air at the eye to measure its pressure. Another method is the I-Care tonometer which bounces a tiny probe off the surface of the eye. Naturally the “tighter” the eye the faster the probe bounces back. All these methods do have variance and it’s the experience of your eye doctor whichever method he uses to take a call on it.
Many studies have found that normal pressure in populations varies between 12 to 21 millimeters of mercury written as mmHg.
However, a large number of people may have pressure higher than 21 and NOT have glaucoma. At the same time, more than 30% of all Glaucoma patients have pressure lower than 21 mmHg.These are called Low or Normal-Tension Glaucoma. These patients in the course of treatment will need their pressure reduced by about 30% from the initial pressure.
Field testing is done on a large unit called an “Automated Perimeter”.This machine shows spots of light at various places on a screen. Inability to see these spots are noted by the machine as field loss and a map is plotted by the computer. This field of vision is a very important indicator of the presence and progression of glaucoma.
In the very late stage of the disease, the patient feels that he or she is looking through a tube as the side vision is gone. This is called tubular vision and is a LATE STAGE of the disease.
The eye doctor will after looking in the eye draw a picture on the paper and write 0.7 cuppings or 0.5 CD ratio, What does this mean.
It means that the ratio of the diameter of the depressed area of the optic nerve to the diameter of the nerve is expressed as a ratio.
Normally cupping in normal eyes is 0.2 to 0.4 and in high minus number eyes, even 0.5 may be normal.
It’s not the initial cupping but DOCUMENTED PROGRESSION that will label an eye as GLAUCOMATOUS.
That’s why the eye doctor writes it after looking in the eye as he or she can compare it to the next visit and see if it progressed.
Non-Penetrating Glaucoma Surgery:
How does modern technology measure and follow up the optic nerve changes.Whats a angio OCT machine ?
The optic nerve changes, today can be measured by a machine called an angio OCT from the USA, which measures the changes and gives a report. This machine creates a map of the nerve behind (just like a physical map of the earth where mountains are denoted as brown and flat areas as green). It uses a color-coding to show which part of the optic nerve is depressed inwards by glaucoma. This is performed every 4 months to know if the nerve changes are progressing or not. In the olden days, the eye doctor would look in and draw a diagram, however today this machine plots for our thousands of points on the nerve which is as small as 3 mm in diameter giving us a much more accurate assessment.
The second detail an Angio OCT checks is the “GCC”.This is the nerve cell layer in the retina which thins out in Glaucoma. This is even more sensitive than a field test and changes to GCC are the FIRST sign of glaucoma.
Also, an Angio OCT can check glaucoma by analyzing the blood flow and capillary network around the optic nerve.
However modern technology or not it cannot replace the doctor’s experience. Angio OCT has been proved to detect glaucoma up to 5 years before field tests and is our new warrior in the fight against Glaucoma.
In some cases, glaucoma can be there without increased pressure, called normal or low tension glaucoma(NTG). It is now known that more than 30% of all glaucoma patients are NTG patients. These normal-tension glaucoma patients’ eyes cannot stand even normal pressure and the pressure needs to be reduced by 30% lower than it is. For example, if a patient has 18 pressure and is diagnosed by the eye doctor with normal-tension glaucoma the pressure will have to be reduced by 30% to 12 to control the progress of the disease.
If we check EVERY patient coming to us with an Angio_OCT we will save hundreds of thousands of people from blindness as using only elevated pressure as a single point detection misses 30 % of all cases.
Glaucoma can sometimes be an emergency when due to the mesh getting totally blocked the pressure suddenly goes to 50 and above. Typically the patient will complain of pain watering and redness and poor vision. This type of acute glaucoma “Attack” is to be aggressively treated with IV injection of mannitol, laser, and eyedrops otherwise it will lead to blindness. As soon as pressure falls we must remove the cataract if it was the cause which it usually is-Do not DELAY!!
Glaucoma can be treated medically or surgically.
Early glaucoma is usually easily treated with just eye drops. These eye drops will have 2 actions.
- Reduce the amount of fluid produced in the eye and or
- Speed up the exit of fluid from the eye by action on the meshwork and other pathways.
Most glaucoma eye drops cause a little bit of irritation and dryness of the eye along with redness and must be used under the doctor’s orders only.
Some eyedrops like Timolol can aggravate a patient’s asthma and some like Prostaglandins cause the skin around the eye to darken and eyelashes in that eye to grow. Do speak with your eye doctor about the side effects of each glaucoma eyedrop.
Rarely when eye pressure does NOT come under control Diamox tablets are prescribed. A common side effect is tingling and numbness in the hands and feet.
Stents:
Since the seventies the most common surgery for glaucoma is Trabeculectomy. In this, a flap is made in the white of the eye, and under that, a hole is cut into the eye from which the fluid flows out.
Problems with this were bleeding, very low pressure, and poor vision after surgery. Such problems led to patients fearing glaucoma surgery and led to many patients losing their sight rather than opting for this surgery.
However, trab. As it’s called for short performed by an expert rarely leads to any problem.
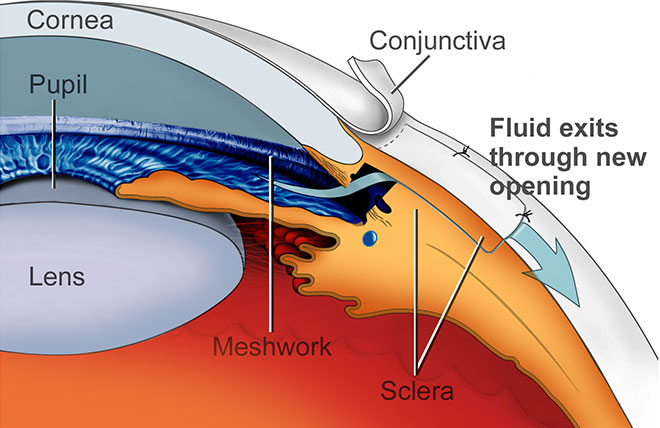
What's a safer alternative to trabeculectomy, What's Non Penetrating Deep Sclerectomy and Canaloplasty ?
In the late nineties, a new procedure came out of Switzerland and western Europe called Non-Penetrating Deep Sclerectomy. Here the eye is NOT OPENED and only the sclera ie the white of the eye is thinned until the fluid canal called canal of Schlemm is opened. The advantage with this is that the pressure is maintained low and there is no chance of bleeding, poor vision, too low pressure, etc. This procedure now is the glaucoma surgery of choice in the west.
Only a few cases where very low pressure is required is Trab still preferred. In India, it still has to catch on. The author began performing this surgery back in 2001 and has reported excellent results with it.
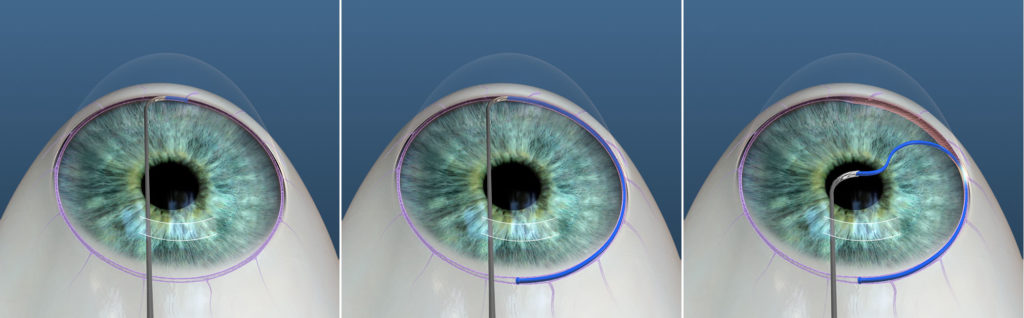
Canaloplasty:
 P
P
In cases where a Trab or other Glaucoma surgery is bound to fail like High diabetics, Neovascular Glaucoma, etc laser energy is applied directly to the ciliary body. This decreases the production of the fluid called aqueous. This naturally decreases the pressure in the eye.
In cases where all surgery will not work and pressure is persistently high a device called a Glaucoma valve is fitted. If well fitted it usually reduces pressure and works well. However, its downside is that sometime in the future it may get choked and require cleaning(simple outpatient procedure), and it’s expensive 400$ and up.
Incidentally, one of the most popular valves was designed by Ahmed and is called the Ahmed Valve. Another commonly used one is the Barveldt valve. We have published good results with the Mehta Valve which is a much more economical alternative optimized for Indian eyes.
What's the advantage of Non Penetrating Glaucoma surgery and Canaloplasty over the Conventional Trabeculectomy Surgery ?
In Non-Penetrating Glaucoma surgery and Canaloplasty, the eye is not opened and only a very tiny passage called Schlemms canal is opened using microsurgical techniques and tiny instruments including lasers. The great advantage of non-penetrating glaucoma surgery over the old conventional glaucoma surgery is that the eye isn’t opened. In traditional glaucoma surgery, there are certain side effects like bleeding. The pressure can remain too low after surgery and because of this, the vision remains very poor after surgery. Cataracts form in a few months after traditional glaucoma surgery.
So Canaloplasty was invented to avoid these side effects. Researchers in Germany and South Africa discovered that by expanding the Schlemms canal with a tiny suture you can lower eye pressure gradually without the side effects involved in opening the eye.
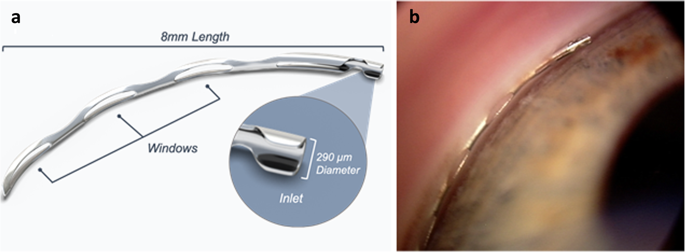
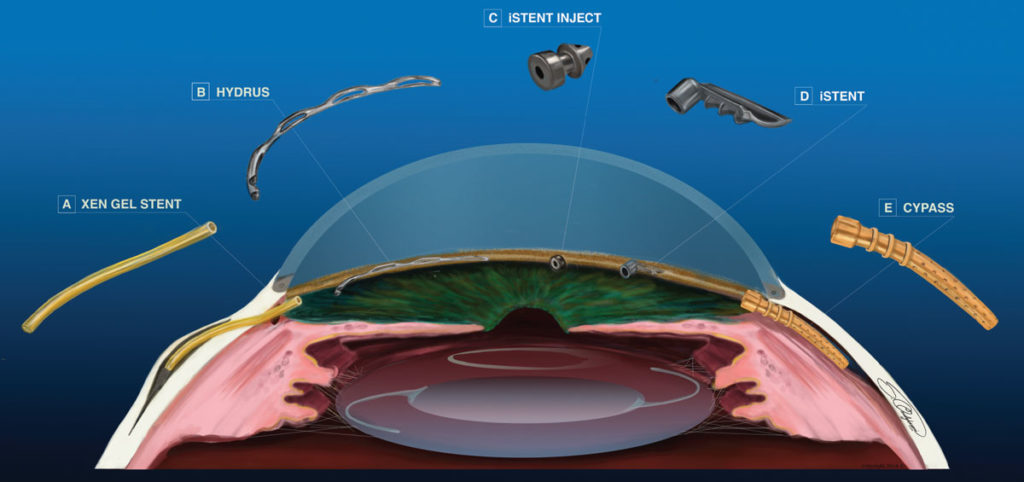
Stents are tiny devices used to keep the Schlemms canal open. They are expensive and so far of questionable value. They aren’t available in India and some have failed the FDA in the USA.
 An instrument that evaluates what you can see with your “field ” of vision from the periphery of your eye while keeping the eye fixated in the middle. It evaluates the extent of the loss. In Glaucoma, the fields progressively decrease till only a central island is left, which if untreated, extinguishes leading to blindness. The Humphrey Analyzer is the Gold standard all over the world. Fields are normally done twice a year. This 842 Analyser is state of the art.
An instrument that evaluates what you can see with your “field ” of vision from the periphery of your eye while keeping the eye fixated in the middle. It evaluates the extent of the loss. In Glaucoma, the fields progressively decrease till only a central island is left, which if untreated, extinguishes leading to blindness. The Humphrey Analyzer is the Gold standard all over the world. Fields are normally done twice a year. This 842 Analyser is state of the art.
842 Perimeter
 Non-ContactPneumotonometer: Acts as an analyzing tool and excellent as a survey instrument. Reasonably accurate when kept properly granted. The Topcon is perhaps the most sensitive of this genre.
Non-ContactPneumotonometer: Acts as an analyzing tool and excellent as a survey instrument. Reasonably accurate when kept properly granted. The Topcon is perhaps the most sensitive of this genre.
 The Icare tonometer provides accurate and objective intraocular pressure reading for all types of patients.
The Icare tonometer provides accurate and objective intraocular pressure reading for all types of patients.
Optovue Technology Avanti: The New Standard In OCT Imaging For documentation and monitoring of ocular disease.
Avanti: The New Standard In OCT Imaging For documentation and monitoring of ocular disease TREND Analysis providing an assessment of the rate of change for Retinal Nerve Fiber and Ganglion Cell Complex structure. Comprehensive analysis tools for the assessment of changes over time in retinal nerve ber, optic disc parameters, and ganglion cell complex structures.